

By Amanda Just, MS, and David Kennedy, DDS, from CHD’s Partner: International Academy of Oral Medicine and Toxicology (IAOMT)
Fluoridation is the addition of an industrial compound to the public drinking water for the purpose of altering the consumer’s oral health. Municipalities that add fluoride to their water supplies do so based on a “one dose fits all” approach. This blanket approach fails to address the smaller size of infants and children and the larger proportions of water and other fluoridated beverages they drink. Significantly, a formula-fed infant drinks its weight in water every three to four days, resulting in the most vulnerable members of the population consuming by far the largest dose of fluoride.
Fluoridation advocates have acknowledged that fluoride’s predominant effects for growing decay-resistant, harder teeth come from topical use (i.e., applying it directly onto teeth) as opposed to systemic exposure (i.e., drinking or ingesting fluoride through water or other means). However, research also has indicated that fluoride does not aid in preventing pit and fissure decay (the most prevalent form of tooth decay in the U.S.) or in preventing baby bottle tooth decay (prevalent in less affluent communities). In malnourished children and individuals of lower socioeconomic status, fluoride may actually increase the risk of dental caries due to calcium depletion and other circumstances. Given this body of research—and Harvard experts’ warning that fluoride is one of 12 industrial chemicals known to cause developmental neurotoxicity in human beings—why do public health officials persist in claiming that water fluoridation is either necessary or safe?
RELATED STORY:
[Researchers] found that the reasonable maximum exposure estimates exceeded the upper tolerable intake and concluded that some children may be at risk for fluorosis.
Overexposure and Dental Fluorosis
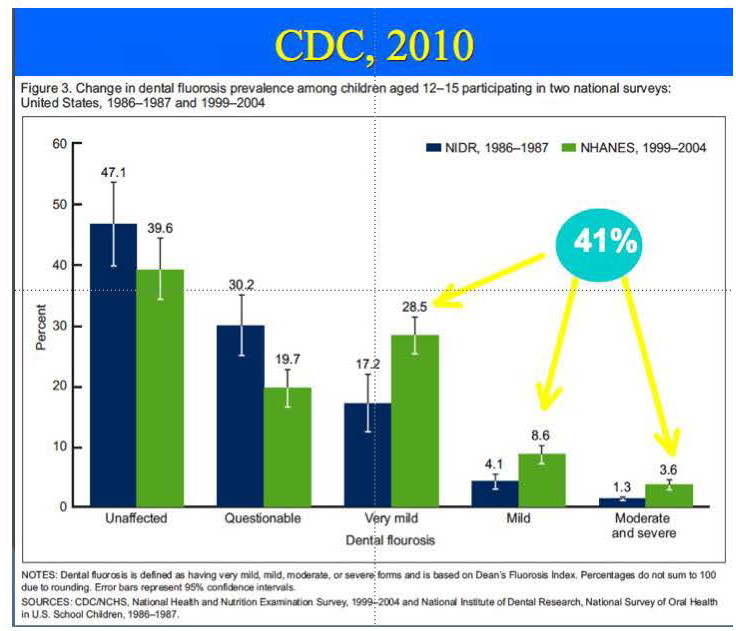
Exposure to excess fluoride in children is known to result in dental fluorosis, a condition in which the tooth enamel becomes irreversibly damaged and the teeth become permanently discolored, displaying a white or brown mottling pattern and forming brittle teeth that break and stain easily. Dental researchers have identified dental fluorosis as a first sign of fluoride toxicity.
According to data from the Centers for Disease Control and Prevention (CDC) released in 2010, 41% of children aged 12-15 exhibit fluorosis to some degree, up from 23% of 12-15-year-olds in 1986 (see figure below). These increases in rates of dental fluorosis were a factor in the U.S. Public Health Service’s 2015 decision to dramatically lower its water fluoridation level recommendations, from a high of 1.2 milligrams per liter (mg/L) down to 0.7 mg/L.
The downward revision of the Public Health Service’s recommendations for fluoride concentrations in drinking water fails to account for the fact that children are exposed to many different sources of fluoride on a daily basis. Exposure to these diverse sources has drastically increased since community water fluoridation began in the U.S. in the 1940s. In addition to water and other beverages, fluoride exposure occurs through food, air, soil, dental products used at home and in the dental office, and through an array of other sources.
RELATED STORY:
Several studies conducted in the United States have offered data about children’s exposure to multiple sources of fluoride, as well as warnings about the situation. Markedly, a study published in 2015 by researchers at the University of Iowa considered exposure from water, toothpaste, fluoride “supplements” and foods. The researchers found that there was considerable individual variation in exposure levels and offered data showing that some children exceed the alleged “optimal” range. Highlighting the problematic nature of issuing recommendations about fluoride intake, the authors concluded:
[I]t’s doubtful that parents or clinicians could adequately track children’s fluoride intake and compare it [to] the recommended level, rendering the concept of an “optimal” or target intake relatively moot.
A similar 2005 study by researchers at the University of Illinois at Chicago evaluated children’s fluoride exposure from drinking water, beverages, cow’s milk, foods, fluoride “supplements,” toothpaste swallowing and soil ingestion. They found that the reasonable maximum exposure estimates exceeded the upper tolerable intake and concluded that “some children may be at risk for fluorosis.”
… research completed by Dr. Elise Bassin while at Harvard School of Dental Medicine showed that exposure to fluoride at ‘recommended’ levels correlated with a seven-fold increase in osteosarcoma in boys who had been exposed between the ages of five and seven.
Pediatric Cancers and Fluoride
In 2006, the National Research Council (NRC) issued a report discussing the potential link between fluoride exposure and osteosarcoma. This type of bone cancer is one of the most common groups of malignant tumors in children and adolescents. The NRC stated that while the evidence was as of yet tentative, fluoride appeared to have the potential to promote bone cancers; the authors also cited biological plausibility due to “fluoride’s deposition into bone and its mitogenic effects on bone cells.” A mitogen is a chemical substance that triggers cell division (mitosis)—and cancer represents mitosis that has run amok.
While some epidemiological studies have failed to find an association between fluoride and osteosarcoma, research completed by Dr. Elise Bassin while at Harvard School of Dental Medicine showed that exposure to fluoride at “recommended” levels correlated with a seven-fold increase in osteosarcoma in boys who had been exposed between the ages of five and seven. Bassin’s research, published in 2006, is the only study about osteosarcoma that has taken age- and sex-specific risks into account.
… discussion has ensued as a result of several research studies published in 2018 that linked fluoride to underactive thyroid, attention-deficit/hyperactivity disorder (ADHD) and other adverse impacts on health and behavior.
Other Adverse Impacts
A large number of studies associate fluoride with loss of IQ. For example, a landmark study published in 2017 (funded by the National Institutes of Health) found that prenatal fluoride exposure was strongly associated with lower scores on tests of cognitive function in the offspring. Interestingly, silicofluoride—the fluoride compound used in the vast majority of water fluoridation schemes—has been associated with higher blood lead levels in children, and lead is known to lower IQ. Lead has also been linked to violent behavior, and research likewise supports the potential association of silicofluoride with violence.
Meanwhile, discussion has ensued as a result of several research studies published in 2018 that linked fluoride to underactive thyroid, attention-deficit/hyperactivity disorder (ADHD) and other adverse impacts on health and behavior.
Protect our Children, Protect our Water
While adding a developmental neurotoxin to the water supply endangers everyone in the community, infants and children are obviously at highest risk for harmful effects. In addition to the potential adverse outcomes for this susceptible population discussed above (cancer, IQ loss and thyroid dysfunction), water fluoridation poses other health risks such as arthritis, bone fractures and learning disorders. We need to protect our children—and protect our water—by learning the facts and demanding policies that reduce and eliminate avoidable sources of fluoride, including artificial water fluoridation.
*Article originally appeared at Children’s Health Defense. Reprinted with permission.







{kind=link}